

Introduction
Collegiate Emergency Medical Services (EMS) providers often enter the field with limited or no prior clinical experiences, relying heavily on “on-the-job training” through direct patient care to build proficiency in EMS skills introduced in the classroom. While direct patient care remains a cornerstone of EMS education, simulation-based learning serves a critical supplement by offering providers a low-risk environment to develop and refine skills. This approach not only reduces safety risks to patients but also helps standardize clinical exposure across providers.1
Although some collegiate EMS agencies operate as transport services, many, including Intra Collegiate Emergency Medical Services (IC-EMS) at Indiana University Bloomington, are non-transport, standby-based agencies.2 These agencies primarily provide services for on-campus events, where call volumes are typically low, limiting exposure to patient care. IC-EMS offers a training model that other collegiate EMS agencies can adapt to enhance provider confidence and clinical competence. The agency is a state-certified Basic Life Support (BLS) organization consisting of Emergency Medical Technicians (EMTs) and First Aid (FA) Providers. EMTs are required to hold Indiana state reciprocity and the American Heart Association (AHA) BLS certification, while FAs are required to hold AHA FA and AHA BLS certifications. Although some IC-EMS providers work part-time for local 911 services, the majority gain clinical experience primarily through their role with IC-EMS.
At a minimum, each event staffed by IC-EMS includes one EMT field supervisor, 1-2 EMTs, and 1-2 FAs, with the number of personnel varying depending on the event. Larger events, such as football games, require multiple crews. While IC-EMS staffs many events throughout the year, exposure to high-acuity patients is limited. In the 2024-2025 academic year, IC-EMS had 211 patient contacts, 74% of which were managed at the FA level.
Given this limited exposure to high-acuity patients, simulation-based EMS education is essential for reinforcing clinical skills and preparing providers for real-world scenarios. Simulation-based learning can be used in two ways: to develop foundational skills in newer providers and to challenge experienced providers with complex or infrequent scenarios.5 Simulations can be particularly effective for practicing high-acuity prehospital scenarios that are less commonly encountered in the field, known as high-risk, low-frequency events.3 Simulation-based learning can be adapted based on available resources, including high-technology manikins, simulated patient actors, task trainers, or virtual reality and computer-based simulations.1 A hybrid approach using both patient actors and manikins can allow educators to assess a provider’s communication skills with patients while also testing clinical skills, such as starting an intravascular line on a nearby task trainer, that cannot be simulated with patient actors alone. Simulation-based learning has been shown to enhance clinical skills, improve problem-solving and critical thinking in challenging situations, boost confidence in decision-making, and strengthen communication and teamwork. Collectively, these benefits contribute to improved patient outcomes.1
This review outlines the training curriculum used by IC-EMS to enhance provider competence, confidence, and field preparedness, offering a model for other collegiate EMS agencies to adopt similar educational practices.
Supervisor Credentialing
IC-EMS staffs every event with a field supervisor, an experienced EMT who oversees operations and leads general member volunteers. To ensure consistent, high-quality care across providers from diverse training backgrounds, IC-EMS has developed a comprehensive supervisor credentialing process to determine baseline provider competency and leadership readiness. This is particularly important given the agency’s student-run, volunteer-based structure with rolling admissions, resulting in a high proportion of new and lesser experienced providers.
The credentialing process begins with a one-day training outlining supervisor expectations, operational protocols, event preparation, patient documentation, and medication administration according to IC-EMS protocols. Following this foundational training, each prospective supervisor schedules a 1:1 skills check-off session with the Deputy Chief of Education and Division Chief of Training. This session includes both verbal and hands-on assessments, evaluating the supervisor’s response to scenarios such as altered mental status, progressive respiratory distress, chest pain, traumatic injury, and cardiac arrest. Each scenario is graded using a standardized rubric, with candidates being evaluated on a scale from “exceed pass” to “fail.” After each scenario, the supervisor will receive a debriefing, covering key considerations and discussing their performance. This rubric is specifically designed to offer constructive feedback, emphasizing areas for growth rather than penalizing mistakes.
If a supervisor fails any aspect of the skills assessment, remediation is required to ensure they meet the required standards. Remediation includes giving the supervisor an opportunity to identify the points they missed and the reasons behind the errors before the debriefing session. If a candidate fails one or two stations, they will receive a “conditional pass” and must complete same-day remediation with the same scenarios. If a candidate fails three or more stations, they will receive a “conditional fail” and must undergo same-day remediation and must reschedule skills assessment for another day with new scenarios. If the candidate fails all five stations, they will receive a “fail” and will be disqualified from becoming a field supervisor for that academic year.
In addition to the skills assessment, prospective supervisors not currently working for a 9-1-1 ambulance service are required to complete two 12-hour ride-along shifts with the local 9-1-1 transport service. Supervisors who are already working for a 9-1-1 ambulance service outside of IC-EMS service lines must complete one ride-along with the local service. All supervisors must also complete one shadowing shift at an IC-EMS event under the direction of a credentialed supervisor.
This multi-step credentialing process ensures that supervisors are not only proficient in clinical skills and IC-EMS-specific protocols but are also able to effectively communicate, allocate resources, and lead personnel. Supervisors must be able to delegate responsibility to FA providers, communicate with 9-1-1 dispatchers, transport crews, fire or law enforcement agencies, or emergency department physicians, and ensure a smooth transfer of care when necessary. Overall, this process emphasizes honing leadership qualities to ensure supervisors can manage clinical and operational challenges that may arise, particularly since they are often the most experienced provider on scene.
Simulation Training
Throughout the academic year, IC-EMS conducts simulation-based trainings in collaboration with the Interprofessional Simulation Center at the Indiana University School of Medicine – Bloomington. IC-EMS maintains a unique partnership with the medical school which provides access to the simulation center and its associated resources. In return, IC-EMS supports the school by offering clinical and training opportunities for medical students. Additionally, the agency’s faculty advisor serves as the director of the simulation center, further facilitating access to these resources.
For organizations without formal partnerships, collaborations with local training institutions and public safety agencies may serve as effective strategies to enhance training opportunities. Such collaborations can expand access to physical space, equipment, and, importantly, shared expertise. Simulation does not necessarily require high-fidelity manikins; modalities such as tabletop scenarios and task trainers for specific skills (e.g., airway management, medication administration) can provide meaningful learning experiences. Emerging technologies, including artificial intelligence, may further increase the accessibility of simulation-based training by supporting scenario development and structured feedback, particularly in resource-limited settings.4
These trainings allow providers to gain hands-on exposure to high-risk, low-frequency medical emergencies using high-fidelity mannikins equipped with computer-controlled simulator technology. To create effective training experiences, educators establish clear learning objectives before each session and conduct debriefings afterward to assess participant performance and reinforce key takeaways. Simulation scenarios are typically chosen based on incidents that are most relevant to the campus and surrounding 9-1-1 response areas.
One example of a simulation conducted focused on opioid overdose management. The session began with an educator-led lecture on the identifying of opioid overdoses based on environmental and physiological cues and appropriate treatment protocols. Following the lecture, a group consisting of one EMT and two FA providers entered the simulation room, where they encountered a manikin simulating an opioid overdose. Meanwhile, the remaining participants concurrently observed the simulation via live video from an adjacent room. The session concluded with a group-wide reflection and discussion, providing an opportunity to assess decision-making, communication, and teamwork.
The combination of an educational lecture and a hands-on simulation component allows providers to apply theoretical knowledge, identify skill gaps, and reinforce retention. The pre-simulation lecture ensures all participants are on the same page, providing a standardized framework, especially beneficial for FA providers. Random team assignments further enable educators to assess communication, role delegation, and team dynamics across varying levels of experience. By recreating high-pressure scenarios in a low-risk environment, these trainings improve team confidence and preparedness for real-world emergencies.
Annual Simulation Exercise
A major event that IC-EMS provides service for is the annual Little 500 bike race, which boasts an attendance of more than 25,000 fans of varying demographics. Due to the event’s scale, all providers working the race are required to complete a mass casualty incident (MCI) training and the comprehensive day-long simulation exercise. The goal of these training exercises is to present providers with various medical situations they may encounter and provide them the opportunity to reinforce skills and ask questions.
The MCI training begins with a lecture on incident command systems, triage protocols, and mass casualty management, led by an instructor with experience as a former Fire Chief and current EMS Logistics Coordinator. The lecture introduces providers to the Simple Triage and Rapid Treatment (START) algorithm, focusing on rapid patient categorization during mass casualty events. This is followed by a scenario-based practice using the commercially available START victim set. Providers are grouped into teams of three to four and must work together to triage mock patients based on acuity and transport priority. This exercise requires providers to think critically on how to best allocate limited resources and identify those requiring the most immediate and advanced care.
In preparation for real-world medical emergencies, IC-EMS hosts a day-long, immersive simulation exercise at the stadium where the Little 500 event is held. Participants are split into squads of three to four providers, including an EMT, a FA Provider, an uncertified member, or a medical student. Each squad is provided a gear bag and radio. IC-EMS Agency Chief serves as dispatch, directing squads to their patients using cardinal directions. Squads are expected to communicate with dispatch throughout the day to inform of their status. All squads are expected to work as a team, within providers’ scope of practice, to execute patient care. Due to the variety in providers’ EMS background knowledge, the simulation poses a challenge to squad supervisors. They are expected to bridge education gaps by demonstrating clear communication and facilitative leadership.
The exercise includes ten scenario stations spread out around the stadium designed to simulate common medical emergencies that crews may encounter at the Little 500 bike race and at on-campus special events (Figure 1). Each station is equipped with a station educator and patient actors or manikins, including high-technology simulators. At the end of each station, squads debrief with the station’s educator on strengths and weaknesses regarding their clinical decision-making and skills performed. Debrief points are standardized ahead of time to emphasize key teaching points or common errors, ensuring active reflection and reinforcing learning objectives. In addition to the ten patient case scenario stations, there is also a skills station that allows both FA and EMT providers to practice skills focused on managing airway, breathing, and circulation. Midway through the day, all squads are dispatched to a staged MCI. An individual from the first squad dispatched acts as incident command, initiating the incident command system and coordinating the START protocol. This exercise aims to assess providers’ abilities to manage multiple casualties using available resources, delegate tasks and responsibilities, and operate within the command structure.
Overall, this comprehensive simulation exercise is critical in preparing IC-EMS providers for the Little 500 race and other high-attendance special events by reinforcing clinical protocols and promoting teamwork to deliver quality patient care.
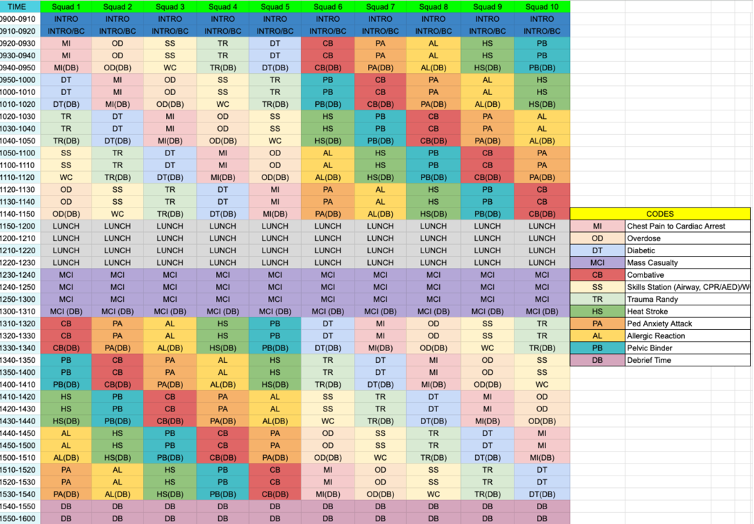
Figure 1. Annual Simulation Exercise Schedule
Future Directions
As a growing EMS organization, IC-EMS is continuously evaluating and improving its education initiatives to maximize both provider development and improve patient outcomes. One of our primary goals is to develop a formalized annual curriculum based on key performance indicators derived from previous year’s quality assurance data. This will allow us to target specific areas for improvement and assess the effectiveness of trainings.
This curriculum will be supported by an expanded and interactive use of the Canvas Learning Management System. Currently, all members are currently enrolled in our Canvas course, which provides access to clinical and operational protocols and practice scenarios. However, we aim to further leverage Canvas through structure modules, including video instruction, quizzes, and discussion boards, to encourage active learning and engagement.
As IC-EMS expands its presence within the community, we recognize the importance of training for the diverse patient populations we may encounter. While our primary patient population consists of college-aged individuals, future training modules will include content focused on pediatric, geriatric, and special needs populations. These additions will help providers better understand how examination, treatment, and diagnosis may vary across different demographic groups.
Furthermore, we plan to incorporate a standardized onboarding process for general member EMTs. This will require the completion of a Canvas module that assesses provider readiness through scenario-based evaluations in areas such as medical, trauma, and cardiac arrest management, as well as protocols for medication administration, equipment usage, and patient documentation. This initiative enhances our current open admissions model by introducing accountability and competency verification in skills and protocols, ensuring all providers are adequately prepared prior to working events.
By leveraging an online educational platform, IC-EMS can provide more flexible and accessible training opportunities, which is especially beneficial for college-aged providers who may have scheduling constraints with in-person events. As many other collegiate EMS programs face similar challenges, implementing structured educational initiatives like these can ensure that all providers are adequately prepared for real-world emergencies.
Acknowledgments
Indiana University School of Medicine – Bloomington, the Indiana University Student Foundation, and other partners for their support of our annual mass casualty drill and trainings.
References
- Elendu, C., Amaechi, D. C., Okatta, A. U., Amaechi, E. C., Elendu, T. C., Ezeh, C. P., & Elendu, I. D. (2024). The impact of simulation-based training in medical education: A review. Medicine, 103(27), e38813.
- Fisher, J., Ray, A., Savett, S. C., Milliron, M. E., & Koenig, G. J. (2006). Collegiate-based emergency medical services (EMS): a survey of EMS systems on college campuses. Prehospital and disaster medicine, 21(2), 91–96. https://doi.org/10.1017/s1049023x00003411
- Mancera, M., Genthe, N., Gussick, M., Lohmeier, M., Thompson, R., & Shah, M. (2022). Acceptability and Preferences of Simulation-Based Continuing Education Among Emergency Medical Service Providers. WMJ : official publication of the State Medical Society of Wisconsin, 121(2), 127–131.
- Rodgers, D. L., Needler, M., Robinson, A., Barnes, R., Brosche, T., Hernandez, J., Poore, J., VandeKoppel, P., & Ahmed, R. (2023). Artificial Intelligence and the Simulationists. Simulation in healthcare : journal of the Society for Simulation in Healthcare, 18(6), 395–399.
- Wheeler, B., & Dippenaar, E. (2020). The use of simulation as a teaching modality for paramedic education: a scoping review. British paramedic journal, 5(3), 31–43.


