
Abstract
Background: Collegiate emergency medical technicians (EMTs) frequently respond to EMS calls with psychiatric emergency components. EMTs can influence whether a patient receives further mental health evaluation and care. However, studies investigating the factors that influence EMTs in such emergencies are limited. Objectives: To investigate how psychiatric emergency call characteristics impacted collegiate EMT decision making at Rice University in Texas. Methods: Rice Emergency Medical Services (REMS) prehospital care reports (PCRs) from psychiatric emergency calls (n=115) from 2011 to 2024 were analyzed, collecting data regarding patient demographics, psychiatric & medication history, call details, call outcomes, and documented referrals to mental health professionals. Results: Patients who were male, under the influence of substances, or not connected with a mental health provider prior to the EMS call were less likely to be informed by EMTs about on-campus mental health resources. Additionally, patients under the influence of substances and those lacking an established mental health provider were less likely to be encouraged to seek further care or successfully establish follow-up plans with a mental health provider after an EMS call. Conclusions: These findings suggest multiple factors influence EMT responses to psychiatric-related calls and help to identify target populations that may benefit from improved follow up.
Introduction
Mental illness and its impact on overall well-being have become increasingly prominent and better understood on college campuses. An increasing number of college students meet the criteria for at least one mental health concern.¹ The 2023-2024 Healthy Minds Study, which surveys over 100,000 college students over the age of 18, reports that 19% of college students meet the criteria for severe depressive symptoms (PHQ-9>=15) and 34% of college students meet the criteria for moderate or severe anxiety symptoms (GAD-7>=10).¹ Additionally, of the students who received positive depression or anxiety screens in the past year, only 61% of these students reported receiving any mental health therapy, counseling, and or psychiatric medication.¹ This sharp rise in incidence of mental illness amongst college students may in part be attributed to an increased awareness and identification of mental health issues in childhood and adolescence, as well as an increased willingness to report mental illness on surveys. Regardless, collegiate emergency medical technicians (EMTs) can play a vital role in recognizing and helping to treat this population.
Collegiate EMTs are uniquely positioned to support members of their college community, as their roles as students as well as EMTs fosters a sense of familiarity and trust among their peers. Furthermore, recent studies have shown that there is a rising trend in the rate of alcohol-related ED visits among young people 20–24 years of age, with 35% of ED visits in this age group having a co-occurring mental illness.² Beyond EMS care, many universities offer free or low-cost therapy services to their students, making their resources reasonable options for most of their students regardless of financial status.³ As such, collegiate EMTs have the ability to connect their university-affiliated patients with these mental health resources and establish continuity of mental health care. Collegiate EMTs are likely one of the first and often only medical professionals a patient on campus will confide in about mental health concerns. As a result, collegiate EMTs can play a critical role in bridging the gap between a patient receiving adequate mental health care and going without necessary support.
Despite the growing incidence of mental illnesses amongst the collegiate population in the United States, collegiate EMTs’ responses and decisions in EMS calls with psychiatric emergency components have not been extensively studied in the literature. Biases in the prehospital setting can influence patient care decisions in psychiatric emergencies and can be associated with prematurely closing encounters, delaying or failing to provide necessary exams, and diagnostic overshadowing. In addition, biases may cause a provider to attribute physical symptoms to mental illness without a thorough consideration of other differentials.⁴ The purpose of this study was to identify variables that impacted collegiate EMT decision-making during psychiatric emergency EMS calls. Identifying these variables will allow collegiate EMTs to implement best practices and be aware of factors that influence their decisions when responding to emergency calls with mental health concerns, ultimately leading to better patient outcomes.
Methods
Study design
REMS uses ZOLL® emsCharts® reporting software to store patient charts, called prehospital care reports (PCRs), and call details. Using filtering features on ZOLL® emsCharts®, REMS charts between March 8, 2011 to June 20, 2024 were searched for calls containing a psychiatric emergency component. The inclusion criteria utilized was REMS PCRs with a clinical category (selected by the in-charge who responded to the call) listed as “Psychological/Behavioral/Suicidal,” “Cardiac Related,” “Alcohol Intoxication,” “Ingestion/Poisoning,” “Breathing Problems,” or “Chest Pain” with a behavioral/psychiatric disorder impression category. Charts that met these initial inclusion criteria were then reviewed according to the following exclusion criteria: patient age less than 18, patient status as not an undergraduate, graduate, or faculty member of Rice University, patient pregnant, prisoner, or in police custody. This study was reviewed and approved by the Rice University Institutional Review Board (IRB).
PCR Selection
An inclusion criteria was used to select which charts would be initially reviewed from the REMS database. This inclusion criteria included REMS PCRs with a clinical category listed as “Psychological/Behavioral/Suicidal.” The inclusion criteria also included REMS PCRs with a clinical category listed as “Cardiac Related,” “Alcohol Intoxication,” “Ingestion/Poisoning,” “Breathing Problems,” or “Chest Pain” with a behavioral/psychiatric disorder impression category. Charts that met these initial inclusion criteria were then reviewed for a secondary inclusion criteria that included patients if they were over the age of 18, an undergraduate, graduate, or faculty member of Rice University, not pregnant, not a prisoner, and not in police custody. Charts that did not fit both inclusion criteria were not included in data collection and analysis.
Data Collection
Thirty different variables were extracted for analysis from charts that were included in the study analysis. These variables were chosen to extract the clinical, operational, and mental health components of each case. Patient demographic data including patient age, month and year of the incident, and sex was collected. Race and ethnicity were not collected in this study because race/ethnicity is not recorded in our electronic medical record. Regarding the context of the call, variables including the chief complaint (as reported by the patient or bystander), number of bystanders on scene, whether the patient was determined to have capacity, and disposition (refusal, hospital transport by ambulance, hospital transport by private vehicle, hospital transport by Rice University Police Department, and refusal against medical advice) were collected. Medical information of the patient during the call, including the initial level of consciousness (LOC), initial respiratory effort, presence of drugs or alcohol on scene, and past medical history were collected. Detailed mental health information was also collected (directly from the patient or bystanders) regarding the call, including whether the patient had a known psychiatric diagnosis, whether the patient takes psychiatric medications, whether the patient has an established mental health care provider, whether REMS or police department attempted or successfully contacted on-campus 24/7 Wellness Hotline during EMS call, whether REMS informed the patient of mental health resources on campus, and whether the patient was encouraged and agreeable to make an appointment with a mental health provider after the EMS call by the EMT (collected via manual review of the call activity log, in which providers document all interventions provided to the patient during the call). All data extracted in deidentified format for analysis and stored securely on the Box platform (www.box.com).
Statistical Analysis
Data analysis involved calculating p-values through chi-square tests on R programming. Odd Ratio was calculated on relationships that were statistically significant p-values (p<0.05).
Results
A total of 163 charts met the inclusion criteria for the study across REMS charts from March 8, 2011, to June 20, 2024. Of these charts, 48 were excluded based on the study exclusion criteria, leaving 115 charts for data collection and analysis (see exclusion criteria in study design section). Statistical analyses of the 115 REMS PCRs indicate that patients who were already connected with a mental health care provider prior to the EMS call were significantly more likely to be informed by collegiate EMTs about mental health resources available to them on campus (p = .022). Specifically, patients who were already connected with a mental health provider prior to the EMS call had 2.52 times higher odds of being informed of mental health resources available to them (OR = 2.52, 95% CI [1.13, 5.6]).
Patients who already had a mental health care provider prior to the EMS call were also significantly more likely to be encouraged and agreeable to either make or ensure that they had an upcoming appointment with a mental health care provider following the conclusion of the EMS call (p = .002). Moreover, these patients had 4 times higher odds to be encouraged and agreeable to connect with a mental health provider (OR = 4.00, 95% CI [1.58, 10.12]).
Patients who were under the influence of drugs or alcohol were significantly less likely to be informed by college-based EMT providers about mental health resources that were available to them (p = .002), with an odds ratio of 0.29 (95% CI [0.13, 0.64]) compared to patients who were not under the influence of drugs or alcohol. Likewise, patients who were under the influence of drugs or alcohol were significantly less likely to be encouraged and agreeable to make an appointment with a mental health care provider (p = .013), with an odds ratio of 0.27 (95% CI [0.09, 0.79]) compared to patients who were not under the influence.
Male patients were significantly less likely than female patients to be informed by collegiate EMTs about mental health resources available to them on campus (p = .029). Male patients had 36% of the odds of being informed about mental health resources available to them compared to female patients (OR = 0.36, 95% CI [0.14, 0.92]).
Patients taking psychiatric medication were significantly more likely to be transported for further medical evaluation (p = .015). These patients were 2.65 times more likely to be transported for further care compared to patients who were not on psychiatric medication (OR = 2.65, 95% CI [1.2, 5.86]).
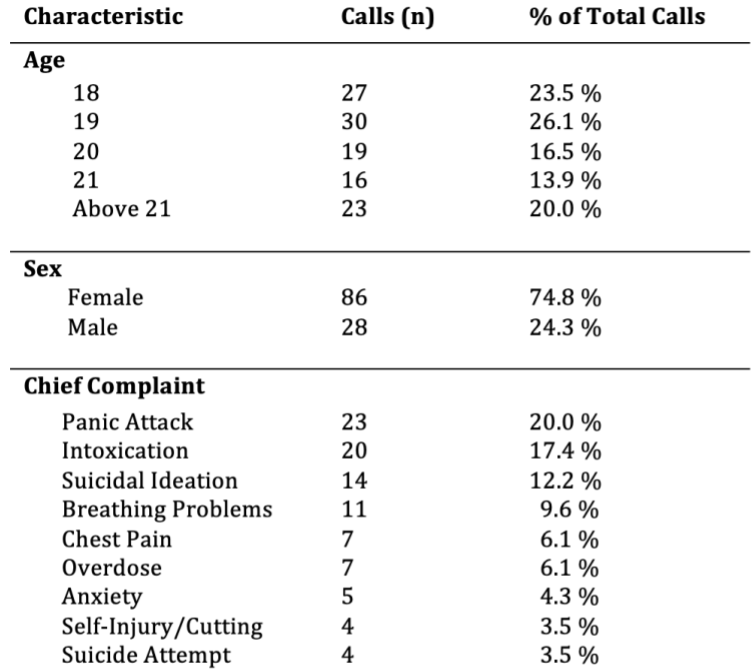
Figure 1. Chief Complaints and Demographics of Emergency Calls: Distribution by Age, Sex, and Presenting Chief Complaint.
Discussion
Our study revealed that collegiate EMTs were significantly more likely to refer patients to additional mental health resources if the patient was already connected with a mental health provider prior to the EMS call. It is possible that it is easier for collegiate EMTs to identify a mental health component to an EMS call if the patient is already connected with a mental health provider. Additionally, bringing up the topic of mental health with patients who are already connected with a provider may be perceived by EMTs as being less likely to cause emotional distress to the patient. Moreover, it is also likely easier for EMTs to ask relevant follow-up questions regarding a patient’s mental health if the patient has already revealed they are engaged with mental health services. Ultimately, awareness of these trends can help EMTs make better decisions for their patients. Though questions surrounding mental health may be perceived as being easier to be asked for any of these reasons, this trend is particularly concerning in cases where EMS is dispatched to cases where mental health components are not extremely apparent.
It is imperative for EMTs to identify such components as it may be a patient’s first and only time of reaching out for help in regards to their mental health. In these cases, it is possible that identifying a mental health component can lead to better patient outcomes because collegiate EMTs are able to refer patients to available mental health resources on campus, often available to university affiliated individuals for free or low-cost.² Collegiate EMTs should ensure that the mental health resources and questions they discuss during an EMS call are not influenced by whether or not the patient is already connected with a mental health care provider.
An important consideration is standardizing the approach to mental health emergencies on campus. Our campus EMS standard operating procedures (SOPs) state providers “can utilize counseling resources for assistance” when responding to psychiatric emergencies. Furthermore, every member of our campus EMS organization undergoes four hours of psychiatric emergency and on-campus mental health resource training as a prerequisite prior to joining the organization. This helps to standardize the treatment approach in each call. Additionally, our SOPs state providers can “utilize QPR for suicidal patients: Question, Persuade, Refer” and encourage providers to ask pertinent questions for psychiatric emergencies. Despite these measures, it is difficult to determine how accurately these SOPs are followed. Standardizing treatment can help to ensure every patient is given resources to follow up after a psychiatric emergency call.
Our study showed that patients under the influence of drugs or alcohol were less likely to be encouraged to seek further mental health care and successfully establish plans with a mental health provider for further care following an EMS call. College campuses generally have a significant number of alcohol-related EMS calls. Studies show that around 17 to 44% of collegiate-based ambulance transportations involve alcohol intoxication.⁵ ⁶ It is well–established that acute alcohol ingestion can contribute to psychiatric emergencies.⁷ Despite Rice’s available resources such as the Rice Counseling Center and the SAFE office (Interpersonal Misconduct and Intervention Support), it is possible that collegiate EMTs do not address mental health components fully with patients under the influence due to difficulty in communicating effectively with intoxicated patients and decreased comprehension from the patient. Additionally, it may be difficult for EMTs to obtain a comprehensive past medical history, specifically a mental health history in patients who are under the influence. However, despite these factors, it is important for EMTs to not overlook mental health in patients under theinfluence. Questions such as “what is your reason for drinking tonight?” and “do you usually drink this amount of alcohol” can start the conversation on any underlying mental health components.
Additionally, a partnership between campus mental health services and campus EMS agencies can implement a streamlined system to follow-up with patients. With this program, if an EMT identifies that there are mental health components to a call, but the patient is under the influence and not able to comprehensively communicate about such issues at that moment, the EMT can leave a mental health resource card which can be used by the patient to follow-up with campus resources the next day. From an EMS-level, it is important that EMTs ask mental health questions and do not overlook intoxicated patients. In the same regard, establishing partnerships between collegiate EMS agencies and campus mental health resources can encourage patients to seek help and recognize resources available to them after EMS calls.
Notably, our study demonstrated that patients taking psychiatric medications were significantly more likely to be transported for additional medical evaluation compared to patients who were not taking psychiatric medications. It is possible that collegiate EMTs recommend transport more strongly because psychiatric medications increase case complexity and may warrant medical resources and services not available in the prehospital setting. Transportation decisions are largely made at the discretion of the provider team and police on scene in collaboration with the patient’s desires. The standard operating procedures (SOPs) stipulate patients who may be a harm to themselves or others, and those without capacity must be transported for further evaluation. Ultimately, EMS transportation to a medical facility during psychiatric emergency calls is a complex decision that requires EMTs to consider factors such as intoxication, agitation, pain, psychosis, and/or other mental illness, and patient and provider safety.⁸ It is important to note that all charts reviewed in this study had a mental health component. Of these charts, approximately 16% involved patients who either recently started a physician-prescribed psychiatric medication or altered the dose of their prescribed psychiatric medication without physician approval. This trend along with leading research suggest that changes in medication regimens can exacerbate mental health problems.⁹ Greater emphasis on understanding patient medication adherence when obtaining patient medical history can help EMTs identify potential mental health components in EMS calls. Specifically, if a patient reports taking a psychiatricmedication such as Fluoxetine or Escitalopram, EMTs should ensure they obtain information on whether the patient takes the medication as prescribed and whether they recently changed their medication dosage, which can support EMTs when deciding the best course of action for a patient.
Our study also revealed that male patients were less likely to be informed of mental health resources available to them compared to female patients. This disparity in mental health information given to male patients may be partially attributed to a combination of societal and cultural influences. Mainly, it is possible that cultural and societal expectations surrounding masculinity discourage male patients from expressing mental health problems they may be facing.¹⁰ For these reasons, male patients may be less inclined to share mental health problems with EMTs, and EMTs themselves may also shy away from the discussion of mental health with male patients. Research on this specific sector of EMS is extremely limited. Additional research on the barriers that male patients feel when discussing their mental health with EMTs can be beneficial. Additionally, research on the barriers EMTs feel they face when discussing the topic of mental health with their male patients can also be beneficial. Currently, EMTs can decrease this disparity between male and female patients by being cognizant of these societal and cultural influences to ensure that they do not avoid topics of mental health with their male patients.
Lastly, of the 115 PCRs analyzed, 3.5% of calls presented with a chief complaint of suicide attempt, 12.2% presented as suicidal ideation, 6.1% presented as overdose, and 20% presented as a panic attack, accounting for 41.7% of the EMS calls analyzed in this study. However, the remaining 58.2% of calls were of chief complaints that did not outright indicate a psychiatric emergency, but ended up having a mental health component. Specifically, 17.4% of calls presented as intoxication, 9.6% presented as breathing problems, and 6.1% presented as chest pain. Hence, while it is important to focus on chief complaints, it is also beneficial to consider other contributing factors as well. It is possible that physical complaints such as breathing problems may be manifestations of an underlying psychiatric illness, highlighting the overlap between mental health and physical health. Recognizing these overlaps is important for collegiate EMTs as they emphasize that the two are not mutually exclusive, highlighting the need for EMTs to be thorough in their questioning and assessment regardless of chief complaint or initial dispatch information.
Limitations
One limitation of the study is the small sample size. A total of 163 charts met initial inclusion criteria, but ultimately only 115 charts were analyzed after applying exclusion criteria. This sample size was sufficient to analyze trends and statistical significance, but limits the study’s generalizability for all collegiate EMS agencies. Future research will benefit from a larger sample size. Moreover, all charts analyzed were EMS calls responding to Rice University and neighboring areas. Rice University is a private institution located in Houston, Texas; therefore, our findings are of limited generalizability given differences in EMT training and campus culture at other institutions. Similar research in other collegiate EMS settings is required to generalize these findings to the general collegiate EMS population.
This study initially used the ZOLL® emsCharts® filtering function to select the 163 charts from the REMS database that were reviewed for analysis. Due to this selection process, only charts where EMTs recognized and documented mental health components were flagged by the filtering function. It is likely that there were cases where collegiate EMTs did not recognize mental health components or did not document such components. Moreover, it is possible that there were PCRs with mental health components, but were not assigned to one of the categories used to filter charts. These charts were not used in the study because they were not flagged by the filtering system.
Due to the retrospective chart review design of the study, the study was dependent on the overall quality and consistency of how REMS EMTs charted. This study focused on REMS charts spanning from 2011 to 2024. In this 13 year span, the REMS Charting Guidelines have been modified multiple times. As such, this likely changed the way charts with mental health components were charted and categorized. Future studies may benefit from standardizing charting across the several years of data analyzed.
Lastly, because the study solely focused on information that had been provided in the charts, there was no way to track long-term outcomes for patients. Specifically, this includes if patients followed through with appointments they were encouraged to make with a mental healthcare provider.
Conclusion
Our data suggests that patients who are already connected with a mental health care provider prior to an EMS call are more likely to be informed by collegiate EMTs about mental health resources available to them. Similarly, these patients are also more likely to be encouraged to seek further mental health care and successfully establish plans with a mental health provider for further care following an EMS call. Additionally, patients who were under the influence of drugs or alcohol are less likely to be informed by collegiate EMTs about mental health resources that are available to them. Likewise, these patients are also less likely to be encouraged to seek further mental health care and successfully establish plans with a mental health provider for further care following an EMS call. Lastly, male patients are less likely than female patients to be informed by collegiate EMTs about mental health resources available to them on campus, and patients taking psychiatric medication are more likely to be transported for further medical evaluation in an collegiate EMS setting.
Considering that these trends were identified in a retrospective case review, it is important that collegiate-based EMS agencies are aware of these findings to promote best practices in responding to psychiatric emergencies on college campuses. We propose that this awareness among EMTs along with partnerships between collegiate-based EMS agencies and campus mental health resources can lead to better patient outcomes in psychiatric emergencies. Additional research on this topic by other collegiate EMS organizations is necessary.
Acknowledgements
We would like to acknowledge the mentorship of Rice University faculty member Ms. Lisa Basgall, EMS director of Rice EMS and Adjunct Lecturer in the Kinesiology Department.
References
-
Eisenberg D, Lipson S, Heinze J, Zhou S. The Health Minds Study (HMS). HealthyMindsNetwork. Accessed February 8, 2025. https://healthymindsnetwork.org/wp-content/uploads/2024/09/HMS_national_report_090924.pdf.
-
Ngo DA, Ait-Daoud N, Rege SV, et al. Differentials and trends in emergency department visits due to alcohol intoxication and co-occurring conditions among students in a U.S. public university. Drug and Alcohol Dependence. 2018;183:89-95. doi:10.1016/j.drugalcdep.2017.10.029.
-
Campus Services are Available When You Need Help. BigFuture. Accessed February 8, 2025. https://bigfuture.collegeboard.org/plan-for-college/get-started/campus-services-there-is-support-when-you-need-it.
-
Crapanzano KA, Deweese S, Pham D, Le T, Hammarlund R. The role of bias in clinical decision-making of people with serious mental illness and medical co-morbidities: a scoping review. J Behav Health Serv Res. 2023;50(2):236-262. doi:10.1007/s11414-022-09829-w
-
Carey KB, McClurg AJ, Bolles JR, Hubbell SJ, Will HA, Carey MP. College student drinking and ambulance utilization. Journal of public health management and practice : JPHMP. 2009. Accessed February 8, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC2958043/.
-
McLaughlin MP. Alcohol-Associated Illness and Injury and Ambulance Calls in a Midwestern College Town: A Four-Year Retrospective Analysis. Prehospital Emergency Care. 2010;14(4):485-490. doi:10.3109/10903127.2010.497897
-
Adès J, Lejoyeux M. [psychiatric emergencies in acute alcoholic intoxication]. La Revue du Praticien. Accessed February 8, 2025. https://pubmed.ncbi.nlm.nih.gov/8134786/.
-
Lowrie LN, Duncan L, Samuels DA, Ablah E, Ofei-Dodoo S. Prehospital clinical decision-making for medication administration for behavioral emergencies. Kans J Med. 2023;16(2):189-193. doi:10.17161/kjm.vol16.20261
-
Neiman A, Ruppar T, Ho M, et al. CDC Grand Rounds: Improving Medication Adherence for Chronic Disease Management – Innovations and Opportunities. Centers for Disease Control and Prevention. November 16, 2017. Accessed February 8, 2025. https://www.cdc.gov/mmwr/volumes/66/wr/mm6645a2.htm#:~:text=Medication%20adherence%20is%20a%20complex,of%20care%20among%20multiple%20providers.
-
Chatmon BN. Males and Mental Health Stigma. American Journal of Men’s Health. 2020. Accessed February 8, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC7444121/#:~:text=One%20of%20the%20areas%20where,about%20his%20or%20her%20symptoms.
Author & Article Information
Nancy Johnson, AEMT, is the current Captain of Rice University Emergency Medical Services (REMS). She is a fourth-year student at Rice University. She is a candidate for a B.S in Neuroscience with minors in Medical Humanities and Spanish. Rohit Gupta, MD, AEMT, is a resident physician at the University of Texas Southwestern Medical Center and serves as an EMS research advisor and adjunct faculty member at Rice University.
Author Affiliations: From Rice University Emergency Medical Services – William Marsh Rice University – in Houston, TX (N.J., R.G.); From University of Texas Southwestern – in Dallas, TX (R.G.)
Address for Correspondence: Nancy Johnson, AEMT | Email: johnson.nancy6043@gmail.com
Conflicts of Interest/Funding Sources: By the JCEMS Submission Declaration Form, all authors are required to disclose all potential conflicts of interest and funding sources. All authors declared no conflicts of interest.
Authorship Criteria: By the JCEMS Submission Declaration Form, all authors are required to attest to meeting the four ICMJE.org authorship criteria: (1) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND (2) Drafting the work or revising it critically for important intellectual content; AND (3) Final approval of the version to be published; AND (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Submission History: Received February 09, 2025, accepted for publication June 23, 2025
Published Online: September 07, 2025
Published in Print: Pending
Reviewer Information: In accordance with JCEMS editorial policy, Original Research manuscripts undergo double-blind peer review by at least two independent reviewers. JCEMS thanks the anonymous reviewers who contributed to the review of this work.
Copyright: © 2025 Johnson & Gupta. This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International (CC BY 4.0) License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. The full license is available at: https://creativecommons.org/licenses/by/4.0/. Cover photo/Featured Photo: © Chalabala/Adobe Stock. Used under license as per author.
Electronic Link: https://doi.org/10.30542/JCEMS.2026.08.01.11

