

Abstract
Background: Collegiate Emergency Medical Services (EMS) differ from non-collegiate services in many ways. This is especially true for smaller collegiate services that lack transport capabilities or advanced life support (ALS) treatment. The decision by non-transporting agencies to request non-collegiate resources may be influenced by factors that transporting services do not have to consider. Objectives: This study aims to determine the factors associated with requests for support from municipal, non-collegiate EMS by collegiate-EMTs. Methods: Retrospective analysis was conducted on 1,230 EMS call logs from a collegiate EMS service. The factors associated with requests for support from non-collegiate EMS are investigated using logistic regression analysis. Results: Altered mental status, reported alcohol use (OR = 3.63, 95% CI: 2.404–5.488), and male (OR = 1.86, 95% CI: 1.313–2.650) or non-binary patients (OR = 3.26, 95% CI: 1.614–6.433) were significantly associated with requests for non-collegiate EMS resources. Conclusion: Many of the factors associated with requests for non-collegiate EMS are also transport indicators for transporting EMS agencies. Increased rates of support requests for male and non-binary patients may be related to sex-based biases seen in healthcare. High rates of support requests for alcohol-related issues demonstrate an area of high reliance on transporting agencies that collegiate EMS agencies could take on.
Keywords: Transport, Logistic Regression, Rural
Introduction
Collegiate-based EMS (CB-EMS systems are widespread in the US, but the vast majority lack transport capability (80%) and ALS (88%)1. CB-EMS agencies that are unable to transport their patients to the hospital rely on NC-EMS to provide transport services. This process alleviates some stress on NC-EMS agencies by allowing collegiate EMTs to provide care to patients who do not require transport, but this places the responsibility to discern whether to request (NC-EMS) support on collegiate EMTs. These decisions are influenced by both clinical and non-clinical factors, such as college policies, campus security personnel, and provider experience and confidence. This research explores the clinical factors associated with the decision to request NC-EMS support. This analysis is primarily descriptive and seeks to understand the factors associated with support requests. It aims to identify opportunities for more efficient cooperation between non-transporting CB-EMS agencies and the external NC-EMS agencies that support them.
Methods
IRB and Ethics Statement
For this study, data were extracted retrospectively from the CB-EMS service call log. The extraction included all EMS calls from January 2015 to September 2024. All data was extracted by an approved service member and was de-identified prior to any analysis being performed. All data points, other than identifying variables, were extracted from the database. Given that the dataset contained case data, additional privacy measures were taken to ensure confidentiality. Primarily, these measures take the form of data suppression. The results, written or otherwise, include only aggregate data, with individual cases being suppressed into tables, figures, or averages. This project was approved by the host institution’s IRB.
Dataset Information
This study used EMS run reports from a small rural college with a non-transporting CB-EMS to identify factors potentially predictive of a request for NC-EMS support. A logistic regression was used to identify those factors that are statistically significant predictors. Requests for municipal NC-EMS are made at the discretion of the responding collegiate EMTs or public safety officers. Public safety officers operate independently but in partnership with the CB-EMS agency. Public safety officers can transport patients following a call, only if they can be released to themselves and require no medical intervention. This service has forty-nine volunteer members, all at the level of EMT. Shifts are assigned on a volunteer basis, with 2 EMTs on duty from 4 pm until 7 am the following day. Some members carry “daytime radios” which allow them to respond to medical calls between 7 am and 4 pm, as they are able. This is known as “unofficial coverage.” Following a medical call, all run reports are submitted to a secure online database for collection and storage. The refusal of service policy is set by the college, which requires a student to be fully aware of the risks of refusal, with no impairment to their orientation.
The dataset contained all EMS calls from January 2015 to September 2024. To account for cases that contained missing data, a multiple imputation approach was used for continuous variables. This approach generates plausible estimates for missing values based on the rest of the dataset. Categorical variables with missing data were simply labeled as “Not Reported”. Patient outcomes are recorded as “release to self”, “released to NC-EMS”, “Transported by public safety”, or “refused care”. Refusal of care cases were removed from the study as they are not relevant to modeling the factors associated with NC-EMS support requests. Those transported by public safety were treated as “Release to Self” cases, as the release criteria are identical in both cases. Public safety officers can only transport a patient after collegiate EMTs have been released to themselves. Collegiate EMTs have no role in the decision-making process to transport by public safety; however, they do report whether it occurred.
Variables were adjusted to fit the limitations of logistic regression. For instance, allergies were transformed into two categories: no known allergies or allergies reported. This was done for any variable that was not already a categorical one. Independent variables included Age, Gender, Airway Status, Circulation, Level of Consciousness (LOC), Skin Appearance, Skin Moisture, Known Allergy, Alcohol Use, Heart Rate, Respiratory Rate, Systolic Blood Pressure, O2 Saturation, Lung Sounds, Blood Glucose, Pupils, Time of Day, Chief Complaint, and EMS coverage level.
Skin moisture was reported as “normal”, “dry”, or “diaphoretic”. This is a qualitative assessment of the skin. The variable of lung sounds, which is an open-ended response in run reports, was classified as one of three levels: “Clear-Bilaterally”, “Abnormal”, or “Not Reported”. Abnormal lung sounds, which include any kind of abnormal noise reported, unilaterally or bilaterally, were combined due to there being only ten instances of these cases. Each pupil can be charted as PERRL (equal, round, and reactive to light), sluggish, fixed-dilated, fixed-constricted, or unreactive. Due to the size of the sample and the lack of sufficient cases in each of these categories, all patients without PERRL pupils were treated as “abnormal pupils”. Level of consciousness is reported as “Alert”, “Responds to Voice”, “Responds to Pain”, and “Unconscious”.
Statistical Analysis
All statistical analysis for this project was done using R Studio v. 4.4.1. Prior to model creation, univariate statistics were calculated for each predictive variable, shown in Table 1. Continuous variables were analyzed for mean values, range, means for cases resulting in release to self and those resulting in request for NC-EMS support, and outcome of a t-test for significance. A Mann-Whitney U-test was used to determine significance in O2 saturation due to the ceiling effect of the measurement (100%). Categorical variables were analyzed for the number of cases for each category, the number of those released to self, and those that resulted in requests for NC-EMS support, and the results of the Chi-Square or Fisher’s Exact Test. Chi-Squared was used unless otherwise denoted. Fisher’s Exact Test was used for variables that contained relatively few cases within a class. The data were then analyzed using a logistic regression, which measures the level of association between variables and a binary outcome. For this regression analysis, the binary outcome was released to NC-EMS or released to self. All p-values < 0.05 are considered to be statistically significant.
Validity Measures
Prior to model creation, the dataset was validated to ensure that the assumptions of logistic regression were satisfied. To assess linearity, all continuous variables were categorized into bins. The proportion of the outcome within each bin was used to calculate the odds and log-odds for each category. Log odds were plotted against continuous variables to visually evaluate whether a linear relationship existed. It was confirmed that an acceptable level of linearity was present for all continuous variables. To ensure independent variables were not highly correlated, a correlation matrix of variables was produced. There were no variable correlations that warranted adjustment or removal from the model. Following model creation, the variance inflation factor (VIF) was used to evaluate multiple-variable correlation. All variables were below the threshold of 5, indicating no significant multicollinearity. Outlier effects were assessed using Cook’s distance. Observations with Cook’s distance values exceeding the threshold of 4/n, where n is the sample size, were reviewed for their impact on the model. No significant outliers were identified that would warrant the removal or adjustment of variables.
Model Development
Using the above independent variables, a regression model was created. This initial model contained all possible variables. The model then underwent stepwise variable selection. After stepwise selection, a final model was created. The final model was then measured for its validity and accuracy. Accuracy was assessed using a prediction test that compared outcomes predicted by the model as compared to actual values. Additionally, a McFadden’s pseudo-R-squared (MF R-Squared) test was used, along with a Homer-Lemeshow test to assess model quality.
Results
1230 CB-EMS encounters were extracted during the studied timeframe. Figure 1 shows the organization and distribution of cases. Out of 1230 cases that were extracted, 1210 were included in the analysis. 119 (~10%) resulted in a request for NC-EMS support. The remaining 1091 (~90%) did not result in NC-EMS support request and were released to themselves.
Figure 1. Case Organization.
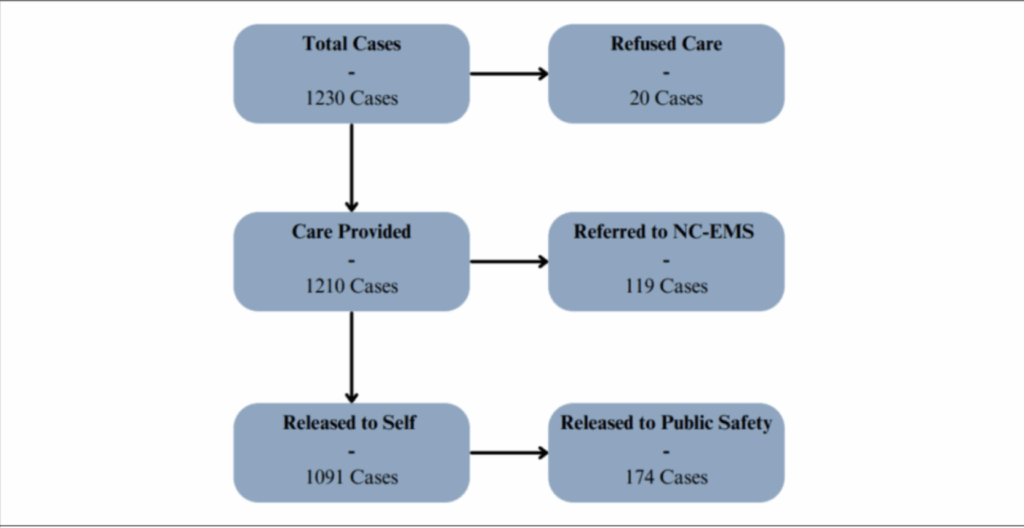
Figure 1. Case Organization. Out of 1230 cases, 1210 were included in analysis. 119 of those cases were referred to NC-EMS. 1091 were not referred to NC-EMS and were released to themselves. Out of those released to themselves, 174 were transported by public safety. These cases were treated as releases to self.
Table 1 shows the results of univariate statistical analysis. Heart rate and oxygen saturation are both significantly associated with the outcome. Higher heart rates and lower oxygen saturation were reported on average for NC-EMS requests. All categorical variables except for known allergy status and blood glucose showed a statistically significant relationship with the outcome.
Tables 1a and 1b.
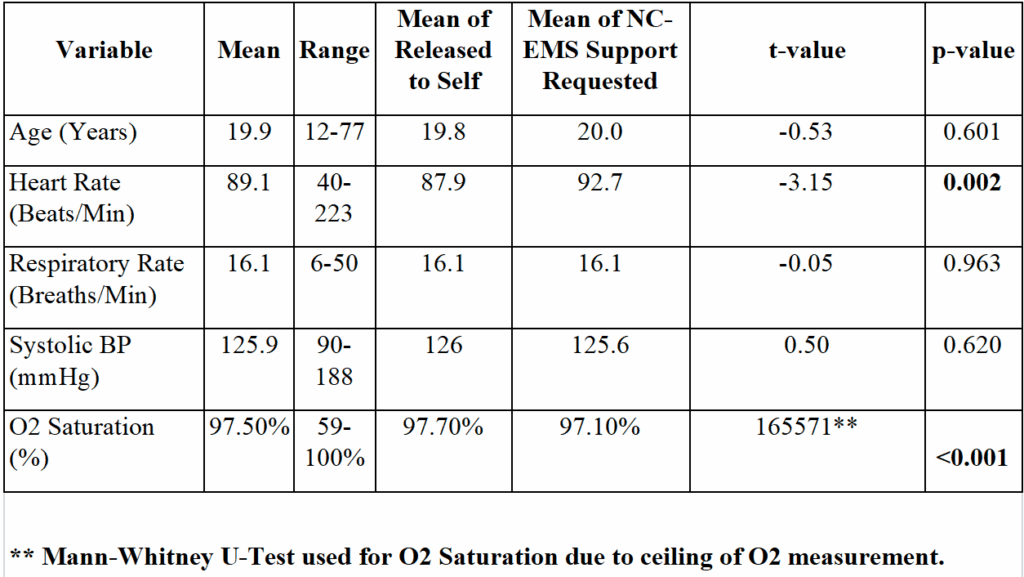
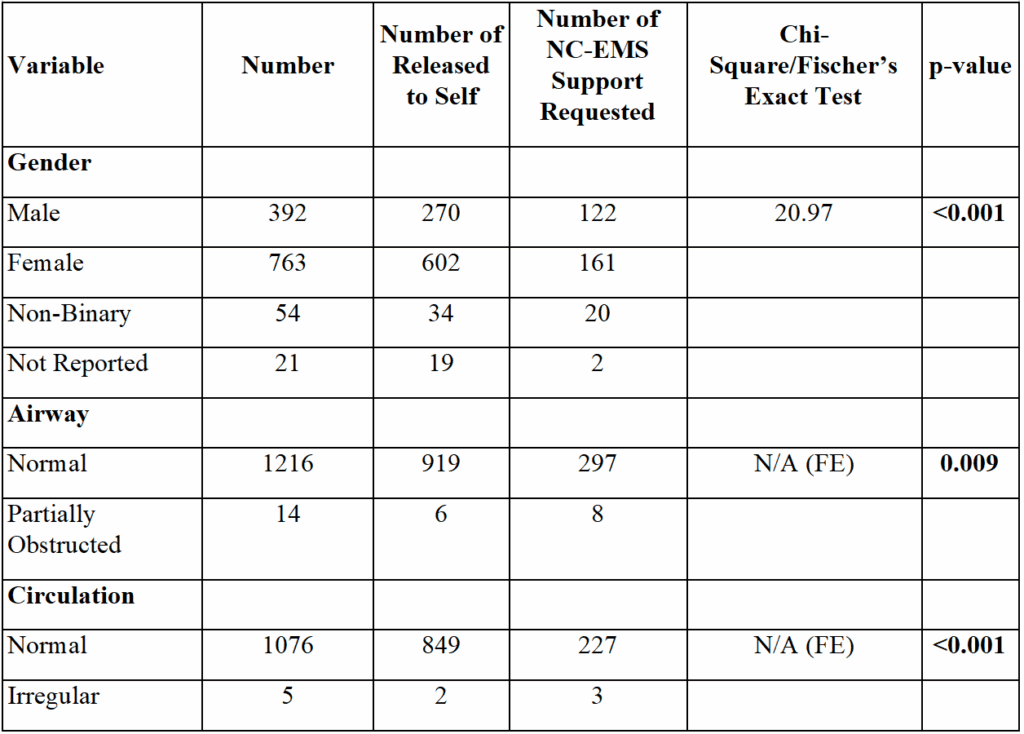
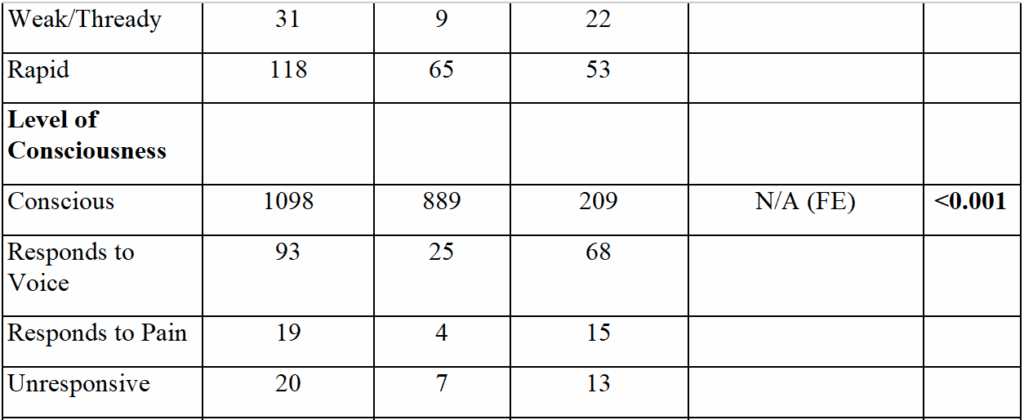
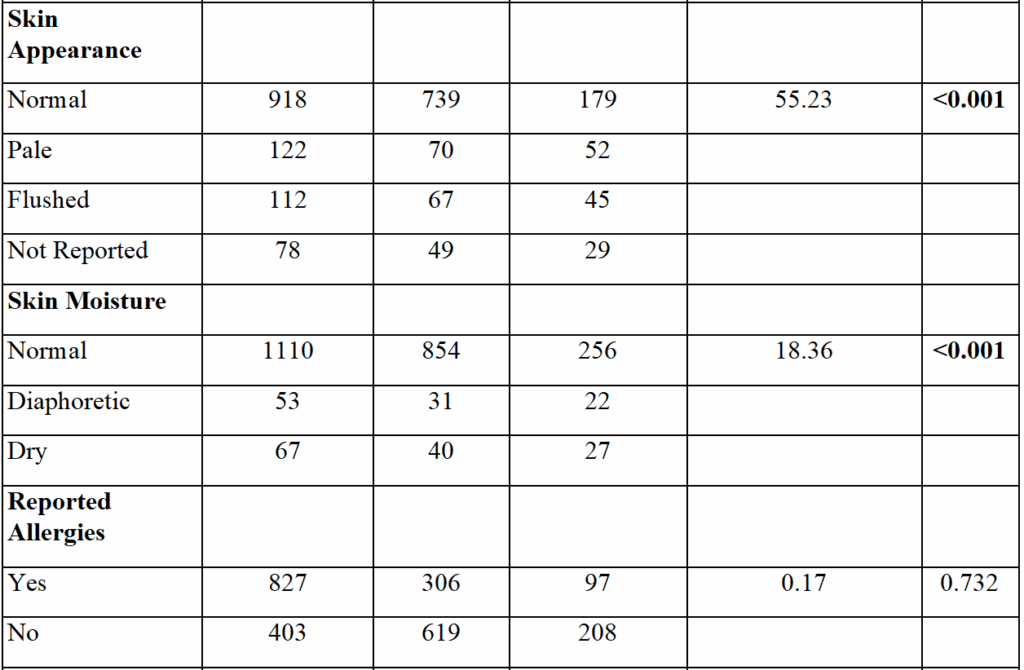
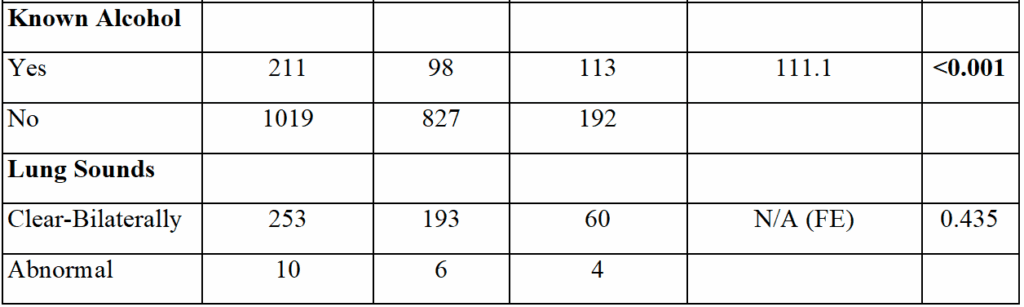
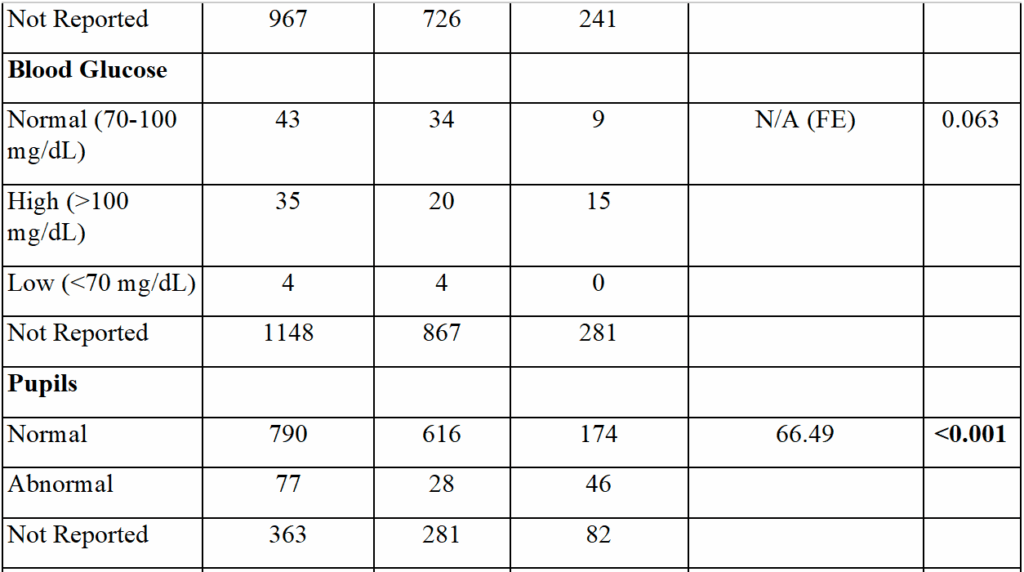
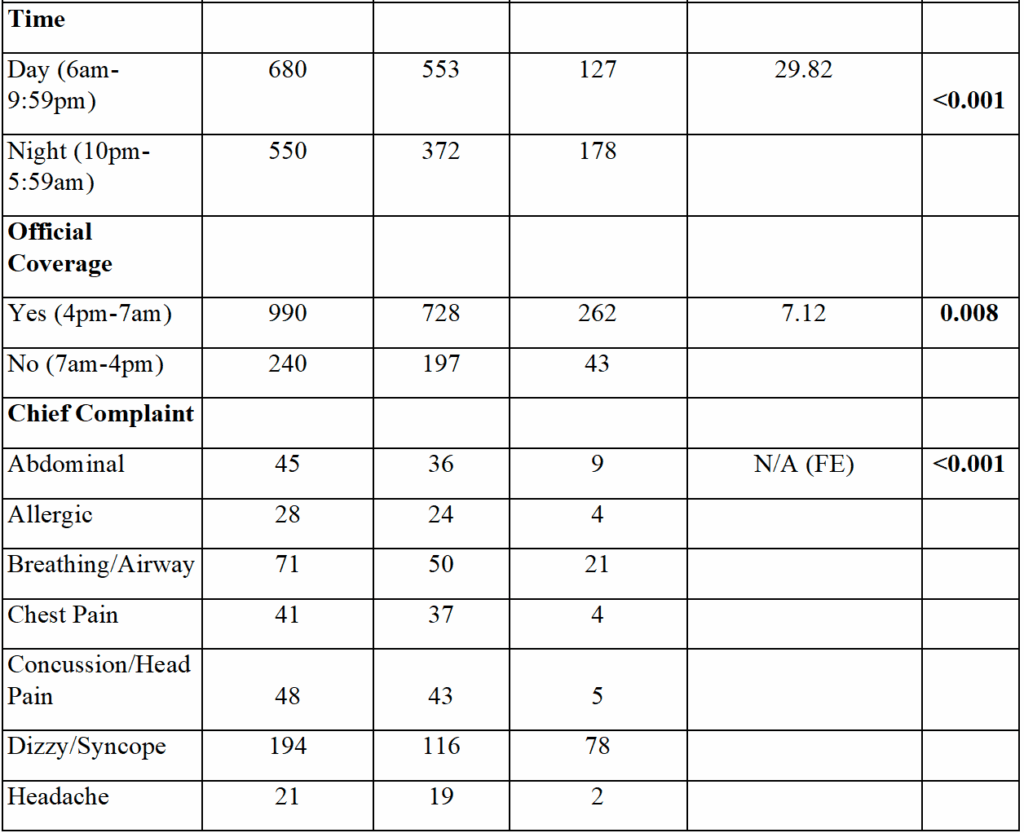
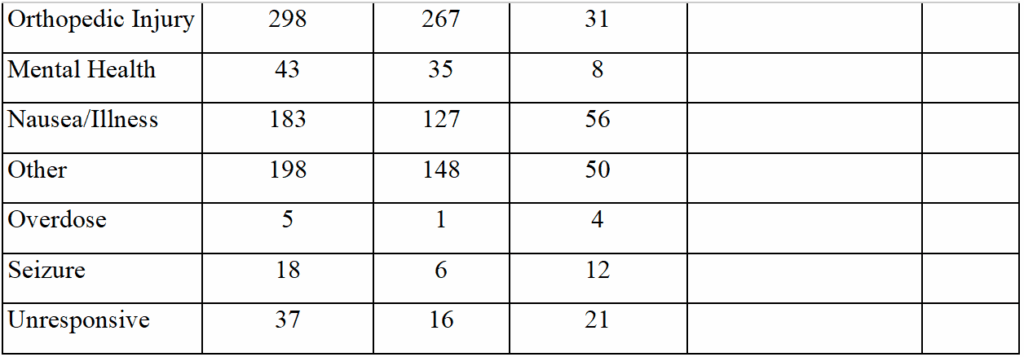

Descriptive statistical analysis showed that female patients were the majority (62%) of patients. The mean vitals within the data set are present within normal physiological ranges. Level of consciousness (LOC), circulation, and airway were predominantly reported as normal. In most cases, neither blood glucose nor lung sounds were reported.
Table 2. Chi Square Analysis of Patient Outcome and Chief Complaint
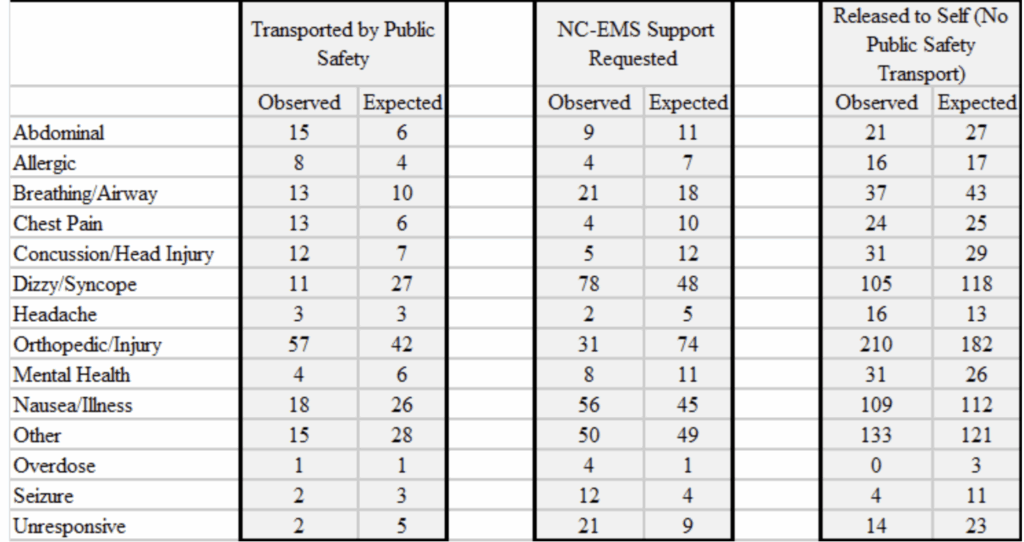

The distribution of chief complaints across patient outcomes was determined, shown in Table 2. Transport by public safety is observed significantly less often for calls reporting the chief complaint of syncope/dizziness, with NC-EMS support being requested for these patients at a higher rate. Abdominal-related calls were transported by public safety at a higher-than-expected rate, however cases involving an illness or nausea were transported less than expected. Orthopedic injuries were overrepresented in the transport by public safety group and released to self group and were underrepresented in request for NC-EMS support group.
Table 3. Logistic Regression Analysis
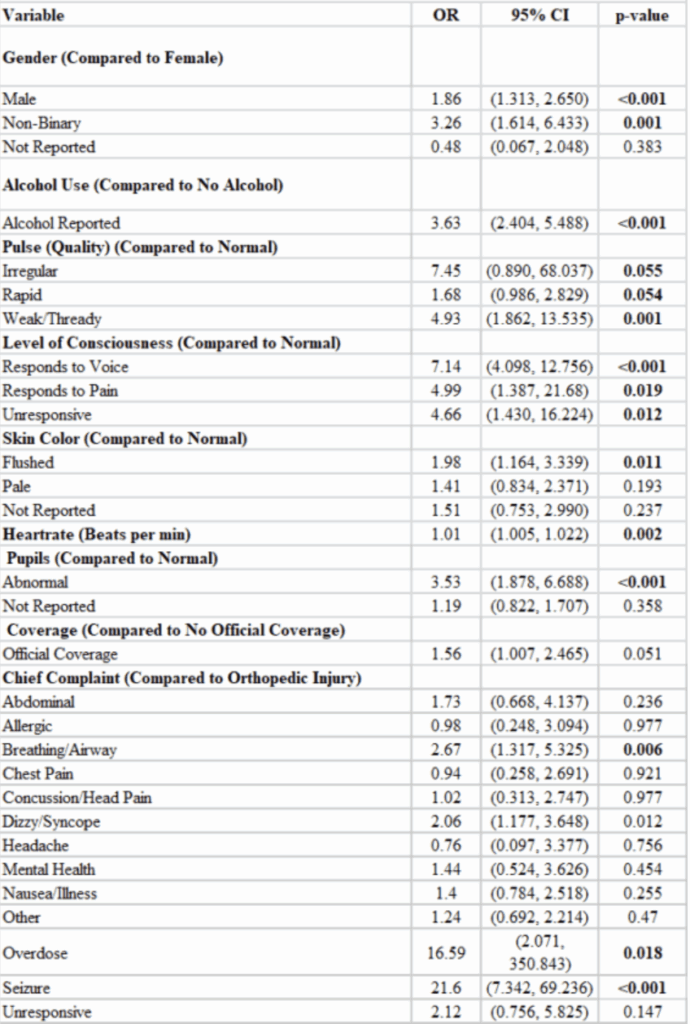

Table 3 summarizes the results of the logistic regression. Significant factors associated with the outcome include gender, with male (OR = 1.86, p = <0.001) and non-binary (OR = 3.26, p = 0.001) patients having a positive association with requests for NC-EMS support. Reported alcohol use was also associated with the request for NC-EMS support (OR = 3.63, p = <0.001). All pulse quality descriptors had a positive association with requests for support compared to normal pulse quality. Level of consciousness was also significantly associated with support requests, with responds to voice (OR = 7.14, p = <0.001), responds to pain (OR = 4.99, p = 0.019), and unconsciousness (OR = 4.66, p = 0.012) as compared to normal level of consciousness.
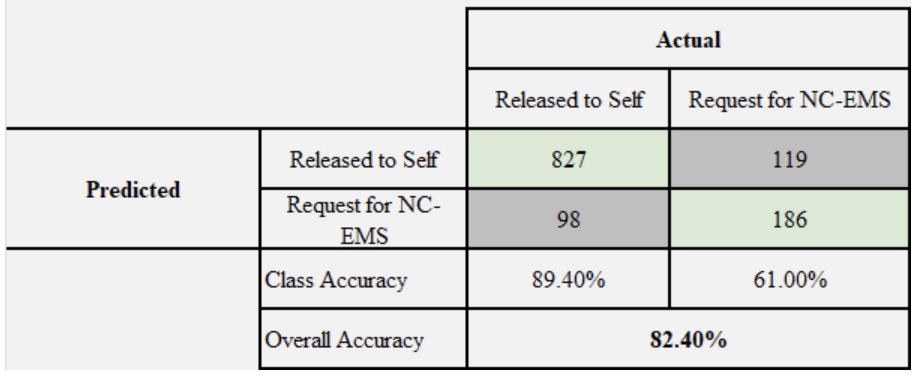
Model accuracy was determined by modeling requests for NC-EMS support decisions using the regression model. These results were then compared to actual outcomes in a confusion matrix. Shown in Table 4, accuracy results show an overall model accuracy of 82.4%. The cut-point for the confusion matrix was set at .35, which is the cut-point that maximized accuracy of the model. The model was more accurate in its prediction of cases that resulted in no support requested from NC-EMS. Additionally, MF R-Squared value was equal to .280, which demonstrates the model is significant at fitting the data.
Table 4. Model Accuracy Results

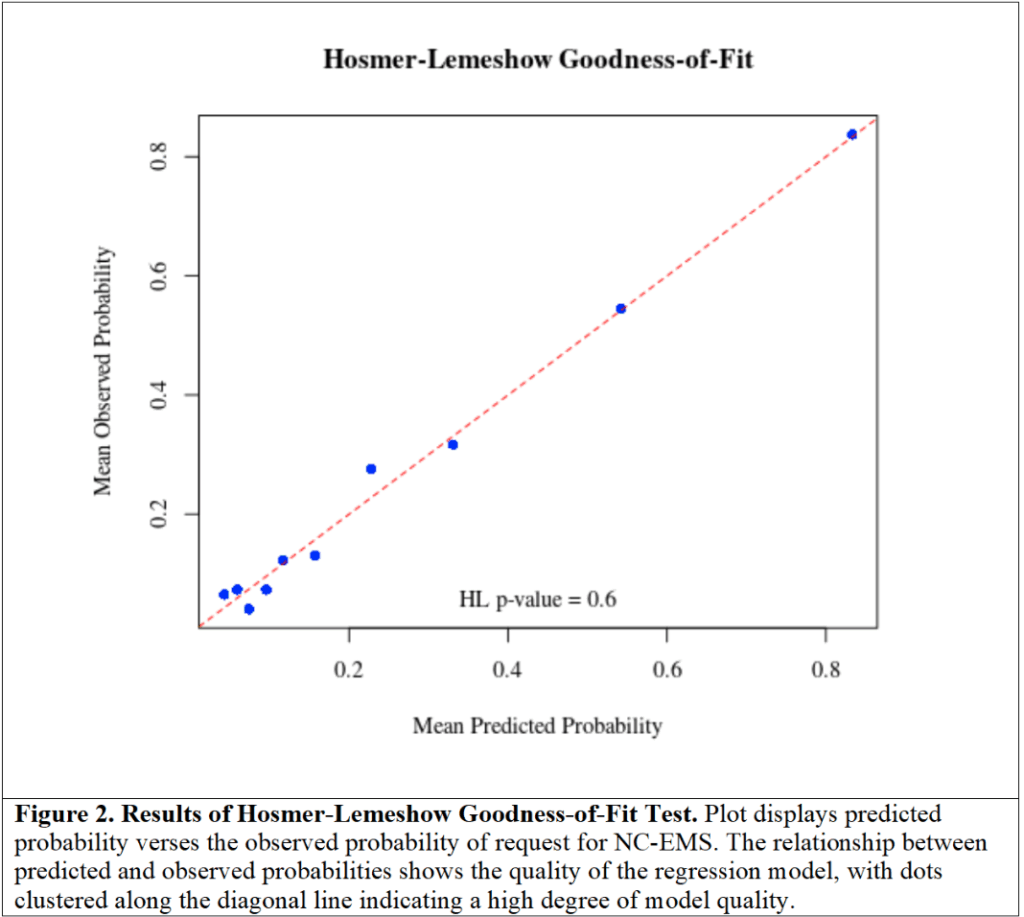
Results of the Hosmer-Lemeshow Test are shown in Figure 2. Points all fall along the diagonal line, which indicate a high-quality model fit (p = 0.6). All methods used to verify model fit and validity indicate that the regression model is significant.
Figure 2. Results of Hosmer-Lemeshow Goodness-of-Fit Test
Discussion
This collegiate EMS agency is a non-transporting, BLS service and covers a campus in a predominantly rural community. Because it lacks transport services, collegiate providers must rely on an outside transporting EMS agency. The transport agency is a non-collegiate, municipal EMS service (NC-EMS). As a rural college campus, the municipal NC-EMS agency is susceptible to the limitations seen in rural EMS, including long transport times, low staffing, and lower funding.² ³
Diminished level of consciousness, chief complaint of seizures or overdose, and indication of alcohol consumption were all positively associated with requests for NC-EMS support. Additionally, it was determined that support was requested for male and non-binary patients disproportionately compared to female patients.
Non-transporting CB-EMS agencies often rely on transporting NC-EMS agencies for patient transport. Therefore, these CB-EMS providers do not make the determination of whether a patient needs to be transferred to a facility for further treatment. Rather, they make the determination of whether additional NC-EMS may be necessary to continue care or provide transport. Cases of request for transport-capable NC-EMS do not guarantee transport. Collegiate EMTs may request NC-EMS support to obtain a second opinion on whether a patient requires transport to a hospital by ambulance. This study investigated factors associated with requests for NC-EMS support by collegiate EMTs.
Level of consciousness (LOC) was strongly associated with NC-EMS support requests. Compared to Alert and Oriented, all other LOC levels (responds to voice, responds to pain, and unresponsiveness) were found to be significantly associated with the outcome. It was also determined that unresponsiveness had the lowest association with support requests. This is contrary to the expectation that patients with the most diminished consciousness, LOC = unresponsive, would have the highest association with NC-EMS support requests. A possible explanation for this phenomenon lies in the charting procedure for the CB-EMS service. Patients presenting with an altered mental status could potentially be labelled as “unresponsive”, despite not meeting the technical standard, which defines unresponsiveness as a complete lack of response to stimulus⁴. Thus, collegiate providers may be mistakenly defining altered and diminished mental status as “unresponsive”. Further inspection of the call log showed that there were at least six patients of the total 19 that were charted as unresponsive and had chief complaints that only specified altered mental status, fainting, or dizziness.
The chief complaint was found to be associated with support requests in the case of seizures, overdoses, and breathing/airway cases. All the other chief complaint categories were not found to be associated with this outcome. This is possible due to the organization of the chief complaint categories, which may group cases of varying severity together. This is not the case specifically for overdoses and seizures, which are very specific chief complaints, whereas abdominal complaints may be more varied in their severity, thus diminishing the significance of their association with an outcome.
Alcohol consumption was seen to be among the strongest associated variables for NC-EMS support requests. The study CB-EMS agency’s guidelines stipulate specific release criteria for patients known to have consumed alcohol. This is due to the diminished level of consciousness associated with alcohol consumption and the requirement for patient orientation to release patients. For a patient to be released to themselves, the collegiate providers must ensure that the patient is A&Ox4 (Alert and Oriented times 4), has stable vitals, has not consumed other dangerous substances, last consumed alcohol at least 90 minutes prior, can walk with a stable gait, and can communicate risks of continued consumption. If these criteria are not met, collegiate providers request NC-EMS support, where custody of the patient can be transferred to the ALS providers.
Cases involving male patients were more associated with NC-EMS support requests, compared to female patients, and non-binary patients had an even higher likelihood of NC-EMS support. The gender distribution of this school is 41.4% male and 56.9% female, with 1.7% identifying as non-binary/non-gender-conforming. It is possible that male and non-binary patients presented with more severe symptoms that were not captured by the regression variables. This is always possible for any regression, as a binary model cannot totally capture the nuance of complex cases. However, there is a known trend of implicit biases in healthcare changing the way in which symptoms are reported and perceived across different genders⁵. Women are more likely to experience discrimination in their healthcare and are also more likely to have their symptoms dismissed⁶. Thus, these factors may be influencing female patients’ forthrightness, which may ultimately impact care decisions. It is additionally possible that non-binary patients experience increased support requests because EMTs exhibit more conservative care decisions due to uncertainty or sensitivity around treating patients with diverse gender identities.
An interaction term was also considered between gender and alcohol usage. Stepwise selection of variables removed any interaction between the levels of either variable. This indicates that both alcohol and gender have a strong impact on model outcomes, independently.
The final regression model has a predictive accuracy of 82.4% overall. However, there is a strong difference in the model’s ability to predict support request cases (61.0%) vs. release to self cases (89.4%). Due to the simplicity of logistic regression, there is a limit on how much nuance can be captured by a regression model. There may be variables outside of the call log that would remedy this predictive gap.
The findings of this study highlight areas that are applicable to other non-transporting CB-EMS agencies. Especially in rural communities, it may be beneficial to reduce the reliance on NC-EMS. In this study service specifically, it may be possible to transport some cases involving alcohol to the local hospital by CB-EMS. This is currently unavailable due to requirements for transporting services to provide mutual aid to the surrounding community. This service currently does not have an ambulance and is unable to respond to medical emergencies in a transporting capacity. It may be beneficial to educate collegiate EMTs on providing care to those with non-conforming gender identities. This research found that these patients were associated with increased requests for NC-EMS support, which may be the result of a lack of confidence from collegiate EMTs in treating these patients. CB-EMS services may also benefit from clear guidelines surrounding requesting NC-EMS to provide consistent and appropriate care to patients.
Limitations
This analysis has limitations in both accuracy and applicability. Much of the nuance of a case was categorized into broad groups for the sake of reducing overfitting. The study sample contained 1230 cases, which, given the number of variables, reduces model specificity. Because the campus is rural and has only one NC-EMS agency supporting it, the results may not be applicable to all collegiate services. The cases from this study spanned a long time frame (2015-2024), during which the service went through growth, both in terms of scope of practice and in terms of the number of members. In recent years, EMTs have begun carrying more medications such as naloxone and epinephrine. There have also been organizational and leadership changes, which may have had an impact on the outcome.
Conclusion
The factors associated with requests for NC-EMS support by collegiate EMTs were analyzed in one non-transporting collegiate EMS agency. Situated within a rural community, both the non-collegiate and collegiate-EMS systems are subject to the limitations that are present in rural healthcare. Some of the factors associated with requests for NC-EMS support include male and non-binary patients, alcohol use, and the chief complaints of seizures, overdose, and airway/breathing-related issues. These factors highlight cases of serious medical emergencies requiring further support from transporting EMS agencies, but they also highlight differences in support requests for patients of different genders. These differences may demonstrate a need for continued education surrounding gender in EMS.
Acknowledgments
The author would like to acknowledge the support provided by Lauren Nicle Gorstein and Sarah Hargett, who provided mentorship through the JCEMS Research Scholar Program. Additional acknowledgement is provided to Dr. Kevin Crisp, who served as faculty mentor for this project.
References
1. United States EMS Organizations. NCEMSF. Accessed November 25, 2024. https://www.ncemsf.org/resources/ems-organization-database/groups-listed-by-region/united-states-ems-organizations
2. Alanazy ARM, Wark S, Fraser J, Nagle A. Factors Impacting Patient Outcomes Associated with Use of Emergency Medical Services Operating in Urban Versus Rural Areas: A Systematic Review. Int J Environ Res Public Health. 2019;16(10):1728. doi:10.3390/ijerph16101728
3. Alruwaili A, Alanazy ARM. Prehospital Time Interval for Urban and Rural Emergency Medical Services: A Systematic Literature Review. Healthcare. 2022;10(12):2391. doi:10.3390/healthcare10122391
4. A systematic approach to the unconscious patient – PMC. Accessed November 25, 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC6330912/
5. Moretti C, De Luca E, D’Apice C, Artioli G, Sarli L, Bonacaro A. Gender and sex bias in prevention and clinical treatment of women’s chronic pain: hypotheses of a curriculum development. Front Med. 2023;10:1189126. doi:10.3389/fmed.2023.1189126
6. eClinicalMedicine. Gendered pain: a call for recognition and health equity. eClinicalMedicine. 2024;69:102558. doi:10.1016/j.eclinm.2024.102558 Anthony Rink, NREMT, is an undergraduate student at St. Olaf College and currently serves as a member of both the St. Olaf EMT Service and Cannon Falls EMS. Rink works as a clinical researcher for a trauma center in Montana. Additionally, Rink was a JCEMS Research Mentee from 2024 to 2025.
Author Affiliations: From St. Olaf Emergency Medical Technicians – in St. Olaf College – in Northfield, Minnesota
Author & Article Information
Address for Correspondence: Anthony Rink, NREMT | Email: anthonyrink17@gmail.com
Conflicts of Interest/Funding Sources: By the JCEMS Submission Declaration Form, all authors are required to disclose all potential conflicts of interest and funding sources. All authors declared no conflicts of interest.
Authorship Criteria: By the JCEMS Submission Declaration Form, all authors are required to attest to meeting the four ICMJE.org authorship criteria: (1) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND (2) Drafting the work or revising it critically for important intellectual content; AND (3) Final approval of the version to be published; AND (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Submission History: Received December 08, 2024, accepted for publication May 05, 2025
Published Online: September 16, 2025
Published in Print: Pending
Reviewer Information: In accordance with JCEMS editorial policy, Original Research manuscripts undergo double-blind peer review by at least two independent reviewers. JCEMS thanks the anonymous reviewers who contributed to the review of this work.
Copyright: © 2025 Rink. This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International (CC BY 4.0) License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. The full license is available at: https://creativecommons.org/licenses/by/4.0/
Electronic Link: https://doi.org/10.30542/JCEMS.2026.08.01.12
Cover photo/Featured Photo: St. Olaf College EMTs © Authorship team.

